



Avulsion
Avulsion
Avulsion is the total displacement of a tooth out of its socket.
Clinical findings
When a tooth is avulsed:
The nerves and blood vessels at the apex of the tooth are severed
The periodontal ligament is torn at the interface between the root and the alveolus
The whole root surface is exposed.
Apical third root fractures are often associated with avulsion. The apical third fragment being retained while the coronal fragment is displaced.
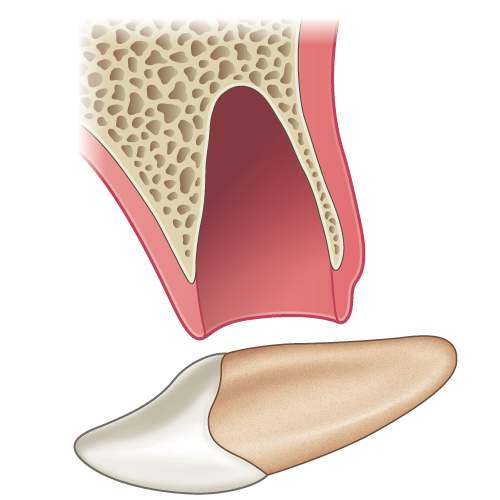
Illustration: Longitudinal section of a tooth showing an avulsion injury.

Labial view of UL1 socket following avulsion.
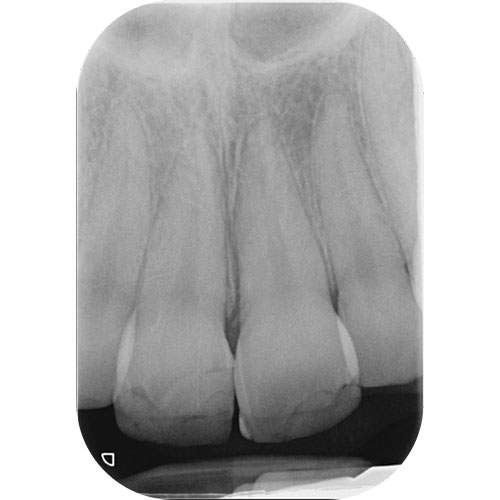
Radiograph of avulsed UL1 socket.

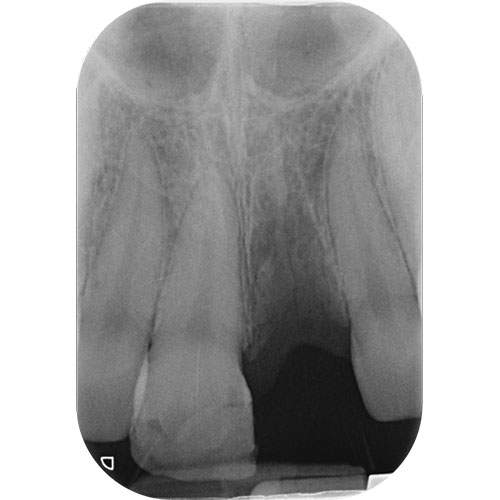
Radiograph of UR1 showing concomitant apical third root fracture with avulsion of the coronal fragment.
Radiographic findings
The radiograph will reveal:
An empty socket.
An associated dento-alveolar fracture if present (seen as radiolucent horizontal lines)
An apical third root fracture fragment retained in situ (seen occasionally).
Management of primary teeth
The general consensus is never to reimplant a primary tooth.
Management of permanent teeth
Depends on:
Stage of root development (whether the avulsed tooth has an open or closed apex)
Extra-alveolar dry time (EADT).
OPEN APEX
For a tooth with an open apex, the aim is to monitor for signs of revascularisation of the pulp space.
If this does not occur and, in the presence of two clear signs or symptoms of pulp necrosis, root canal treatment is indicated.
CLOSED APEX
For a tooth with a closed apex, root canal treatment should be initiated as soon as possible.
Ideally within 7-10 days.
The prognosis is directly related to the extra-alveolar dry time.
IMMEDIATE REPLANTATION
The best long term outcome follows picking the tooth up by the crown and re-inserting as soon as possible, ideally within 15 minutes of the injury. This relies on having knowledgeable and competent personnel at hand who understand the procedure of reimplanting an avulsed tooth.
Once the tooth has been repositioned the patient should bite on a handkerchief and go straight to a dentist.
The dentist will need to verify that the tooth is in the correct position and apply a flexible splint for 2 weeks.
DELAYED REPLANTATION
If the tooth cannot be reimplanted immediately it should be stored in HANKS balanced salt solution or simply in milk. Milk has been reported to maintain the viability of the periodontal ligament cells for up to 6 hours. The patient should then see a dentist urgently.
The tooth should then be rinsed with saline and replanted under local anaesthetic, temporarily held in position, its correct position confirmed with a periapical radiograph.
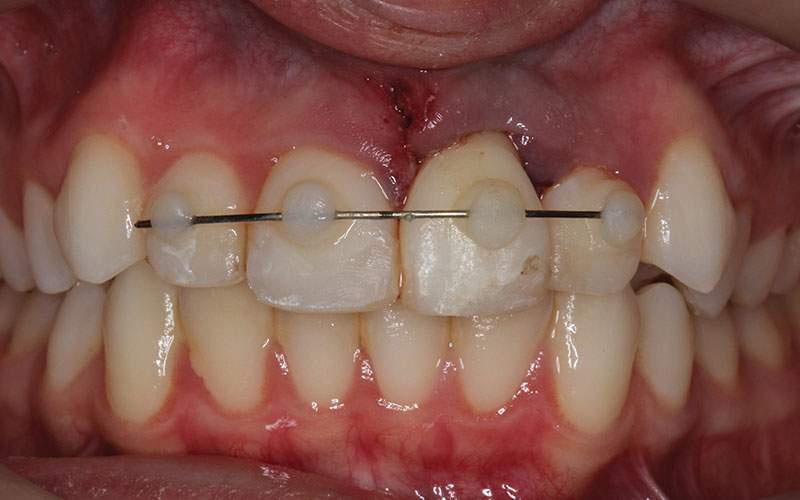
When correctly repositioned it should then be splinted to the adjacent teeth using 0.016″ stainless steel orthodontic wire.

Labial view of repositioned UL1 temporarily held in position with Triad™ (composite can also be used).
Check radiograph of digitally repositioned avulsed UL1.
Labial view of avulsed UL1 following avulsion and subsequent repositioning.

Radiograph showing root filling in avulsed UL1.
Use of systemic antibiotics
The value of systemic antibiotics after reimplantation if still questionable.
If the tooth is replaced immediately no antibiotics are necessary. If there is a delay and thus a chance of infection then antibiotics may be considered.
Guidelines suggest administration of 100 mg doxycycline twice a day for one week in children over 12 years of age and adults – to reduce the risk of root resorption.
Doxycycline should not be used for children < 12 years or in pregnant woman owing to the risk of discolouration of the developing secondary teeth. In such patients penicillin V or amoxicillin or erythromycin (in penicillin allergic patients) should be used.
Endodontic considerations
If root canal treatment is carried out within a few days of the avulsion injury, the canal system should be sterile, and therefore single visit root canal treatment is appropriate.
If there was a risk of a large inflammatory response that would result in a higher chance of resorption, then an intermediate intra-canal dressing should be used. An antibiotic corticosteroid paste to reduce such an inflammatory response can be used, such as Odontopaste. Unlike Ledermix paste this contains clindamycin and therefore will not cause discolouration of the dentine.

Prognosis
There is a growing body of evidence that suggests patients and parents may feel let down if an attempt is not made to replant an avulsed tooth even if the prognosis is considered very poor.
Experts suggest that no matter how poor the prognosis might appear every attempt should be made to replant the tooth.
The aim is to allow bony healing and retention of the tooth until a more predictable approach to tooth placement, ideally with an implant can be undertaken
In the growing patient the replanted tooth could be retained until the patient reaches adult levels of growth and then the implant can be planned
In growing patients there is a high risk of ankylosis with resultant infraocclusion. Careful and diligent monitoring is therefore essential to diagnose this as soon as possible. Referral to a paediatric unit to consider whether decoronation is indicated.
Contraindications to replantation
The following teeth should NOT be replanted:
A primary tooth (as this may cause damage to the underlying secondary tooth)
A permanent tooth in the presence of life-threatening injuries that need attention
A permanent tooth with gross caries or extensive bone loss due to periodontal disease
A medical condition that contraindicates replantation such as severe immunosuppression.
Treatment summary
– Click on each card for a summary –
Verify position, splint for 2 weeks, if apex is closed start root canal treatment within 7-10 days.
Clean root with saline, replant with digital pressure, verify position, splint for 2 weeks, consider antibiotics, if apex is closed start root canal treatment within 7-10 days.