



Online Dental Trauma Guide: Part I Fracture Injuries
Enamel-dentine & pulp fractures
Enamel-dentine & pulp fractures
Involves loss of tooth structure with exposure of enamel, dentine and pulp (also referred to as a complicated crown fracture).
Clinical findings
A tooth with a complicated crown fracture will:
Be sensitive to thermaland tactile stimuli
Be tender to touch
Not be tender to palpation.
Remember labial tenderness could be suggestive of an associated luxation/displacement injury and should be investigated further.
– Ms Serpil Djemal
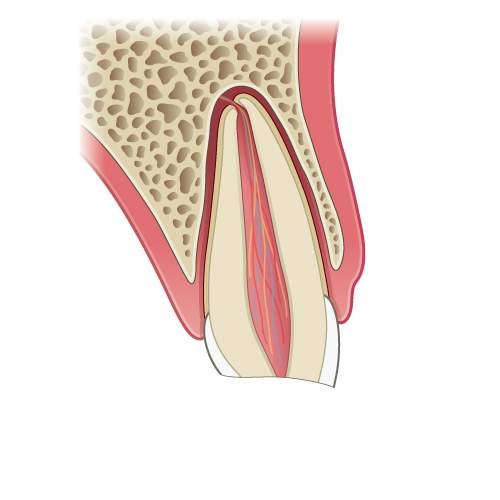
Illustration: Longitudinal section of a tooth showing an enamel-dentine & pulp fracture.

Clinical image: Enamel dentine fracture of the UL1 with pulpal involvement.
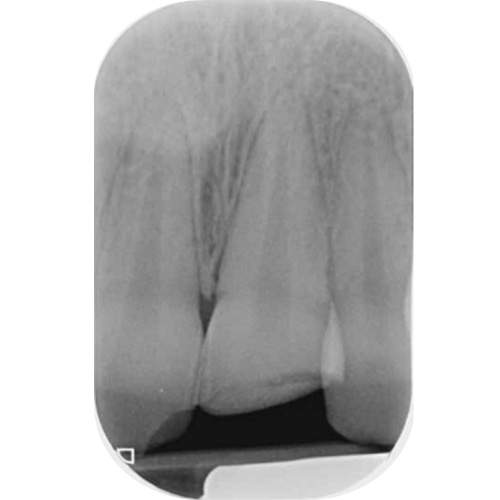
Radiograph: The UL1 showing a normal appearance of the periodontal ligament.
Radiographic findings
The radiograph will show:
Enamel and dentine loss
Breach of the pulp chamber
Normal root and periodontal ligament.
Multiple projection radiographs are advised to eliminate the possibility of root fractures or a luxation injury.
If tooth fragments cannot be accounted for and a lip laceration is present, a soft tissue radiograph is also indicated (see the section on enamel fractures for technique details).
Management
With exposed or near exposed pulps in adults and children, a Cvek pulpotomy should be performed, in the first instance aiming to remove the inflamed superficial pulp. This is particularly important in immature, developing teeth to try to preserve pulp vitality and facilitate root development.
Management of primary teeth
If possible pulp vitality should be preserved with a Cvek pulpotomy
If a Cvek pulpotomy is not possible pulpectomy or extraction may be indicated.
Note: Ideally this should be carried out using rubber dam isolation.



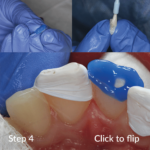



Click on each image above to see the steps for a Cvek pulpotomy
In teeth with closed apices: if the pulp is removed down to the cervical level, then pulp extirpation should be carried out.In teeth with open apices a Cvek pulpotomy should be carried out to the cervical level with the aim of getting continued root formation.
– Ms Serpil Djemal
Radiographic review: at one year
Look for changes in the periodontal ligament space.
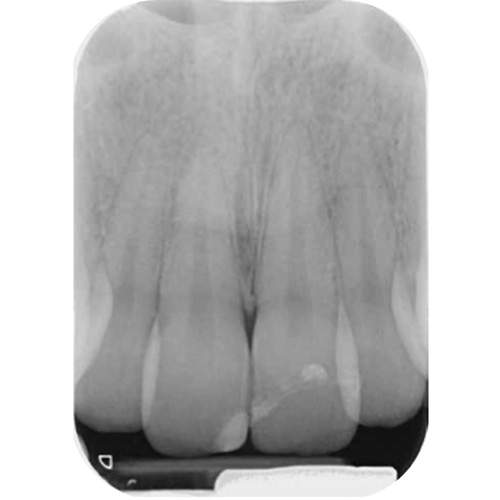
Radiograph: UL1 at one-year review.
Monitoring: Clinical and radiographic review and sensibility testing at 3, 6 and 12 months and then yearly review.