



Online Dental Trauma Guide: Part I Fracture Injuries
Crown-root fractures
Crown-root fractures
A fracture involving enamel, dentine and cementum and may or may not involve the pulp.
Clinical findings
The clinical presentation is variable and the true extent may not be immediately obvious. This will depend on the extent and location and whether the coronal aspect is in one or multiple pieces.
There may be:
Very little mobility and separation of the fractured tooth
Frank mobility and separation of the fractured parts (this is directly related to the depth of the fracture line as it extends palatally)
Tenderness to touch (exquisitely tender on separation of the fractured parts).


Clinical image: Labial view of UL1 suggestive of a crown-root fracture.

Clinical image: Occlusal view of UL1 confirming a crown-root fracture.
It can be very difficult to ascertain the true extent of these types of fractures clinically and the radiographs may be of low diagnostic value. An examination under local anaesthetic allows for pain-free exploration, diagnosis and determination of the full extent of the injury.
– Ms Serpil Djemal
Radiographic findings
The appearance of a crown-root fracture on a periapical radiograph is:
Very variable and may show the fracture line
Often of low diagnostic value.
Multiple projection radiographs may be necessary, including an upper standard occlusal.
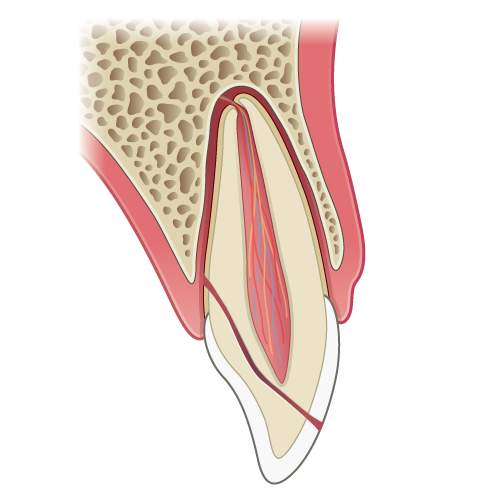
Illustration: Longitudinal section of a tooth showing a crown root fracture.

Radiograph: UL1 showing the fracture line and lost tooth tissue.
Management
Management of primary teeth
Treatment of crown-root fractures in primary teeth involves either removal of the coronal fragment, leaving the root to be resorbed by the successor, or extraction of the entire tooth.
Management of permanent teeth
Treatment of crown-root fractures can vary and is dependent upon the clinical time available and complexity of the fracture. Treatment can take the form of remedial action to make the tooth more comfortable for the patient, providing an intermediate solution and allowing more time for a long-term solution to be planned.
The following treatment options are possible and will be dictated by the extent of the injury:
If the coronal part of the tooth is in multiple pieces and attachment is not possible, root canal treatment and composite build-up may be an option if there is good moisture control (electrosurgery can be very useful)
Re-attaching the fragment with or without pulp management is dependent on good moisture control (electrosurgery may be useful)
Root canal treatment followed by provision of a post-crown
Bonding the fragments together using composite resin can provide a satisfactory stop-gap whilst planning for further exploration
If the tooth is rendered unrestorable and there has been loss of coronal tooth tissue, application of a temporary filling over the tooth/root with glass ionomer and taking an impression for an immediate denture for tooth replacement can be planned.
Treatment options:
Case I: Crown root fracture UL1. Tooth fragment removed, root canal treatment carried out and tooth restored with composite.

Radiograph: UL1 after root canal treatment

Clinical image: Composite build-up of UL1 following root canal treatment.
Case 2: Crown root fracture UR2. Fracture line near gingival margin with fragment being held only by the soft tissues. Composite used to temporarily splint the fragment until more definitive treatment can be planned.

Clinical image pre-treatment: Buccal view of UR2 with a crown-root fracture. Labial fracture line is visible a few millimetres below the gingival margin.

Clinical image post-treatment: Composite veneer placed on UR2 to help ‘splint’ the fragments together temporarily.
Monitoring: The prognosis for crown root fractures is often poor and tooth replacement often inevitable. Follow up will depend on the prognosis of the tooth.